
Posted by FLCCC Alliance
POST-VACCINE TREATMENT PROTOCOL
Management of Post-Vaccine Syndrome
Major public health authorities do not recognize post-COVID-vaccine injuries and no official definition exists. However, a temporal correlation between receiving a COVID-19 vaccine and the beginning or worsening of a patient’s clinical manifestations is sufficient to diagnose a COVID-19 vaccine-induced injury, when symptoms are otherwise unexplained by concurrent causes.
Since there are no published reports detailing how to manage vaccine-injured patients, our treatment approach is based on the postulated pathogenetic mechanism, clinical observation, and patient anecdotes. Treatment must be individualized according to each patient’s presenting symptoms and disease syndromes. Chances are, not all patients will respond equally to the same intervention; a particular intervention may be life-saving for one patient and completely ineffective for another.
Early treatment is essential; the response to treatment will most likely be attenuated when treatment is delayed.
About this Protocol
This document is primarily intended to assist healthcare professionals in providing appropriate medical care for vaccine-injured patients. Patients should always consult their healthcare provider before embarking on any new treatment.
For Additional Potential Treatments, Disease-Specific Therapeutic Adjuncts, and References please see the complete guide, ‘An Approach to the Management of Post-Vaccine Syndrome.’
Patients with post-vaccine syndrome must not receive further COVID-19 vaccines of any type. Likewise, patients with long COVID should avoid all COVID vaccinations.
First Line Therapies
(Not symptom specific; listed in order of importance.)
-
Intermittent daily fasting or periodic daily fasts
Fasting stimulates the clearing of damaged cells (autophagy), damaged mitochondria (mitophagy), and misfolded and foreign proteins. Fasting is contraindicated in patients younger than 18 (impairs growth), malnourished patients (BMI < 20 kg/m2), and during pregnancy and breastfeeding. Patients with diabetes, gout, or serious underlying medical conditions should consult their primary care provider before beginning fasting, as changes in medications may be required and these patients require close monitoring.
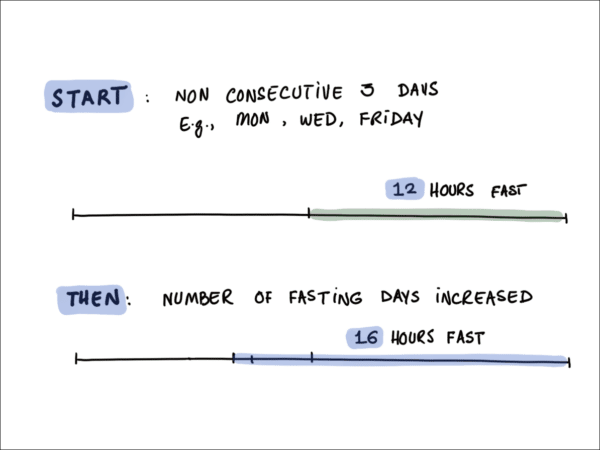
Several studies have suggested that intermittent fasting may not be as beneficial for pre-menopausal women as it is for men. To reduce any adverse effects, women should take a mild approach to fasting: shorter fasts and fewer fasting days. We would suggest beginning a program of time-restricted eating consisting of fasting for 12 hours for two to three days a week (see below) and increasing from there. Furthermore, the fasting window should begin at least 4 hours before going to sleep.
An Intermittent Fasting Plan for Pre-Menopausal Women
For more detailed information see ‘An Approach to the Management of Post-Vaccine Syndrome.
-
Ivermectin: 0.2-0.3 mg/kg/day
Ivermectin, which has potent anti-inflammatory properties, binds to the spike protein and aids in its elimination. It is likely that ivermectin and intermittent fasting act synergistically to rid the body of spike protein. Ivermectin is best taken with or just following a meal for greater absorption. A trial of ivermectin should be included in the first-line treatment approach. The duration of treatment is determined by the clinical response. In patients with a suboptimal response, a trial of a higher dose (0.6mg/kg day) can be considered. If no improvement is noted after 4-6 weeks, the drug should be stopped. Due to the possible drug interaction between quercetin and ivermectin, these drugs should not be taken simultaneously (i.e., should be staggered morning and night). The safety of ivermectin in pregnancy is uncertain, therefore this drug should be avoided in the first trimester of pregnancy. -
Moderating physical activity:
Patients with long COVID and post-vaccine symptoms frequently suffer from severe post-exertional fatigue and/or worsening of symptoms with exercise. Aerobic exercise is reported to be one of the worst therapeutic interventions for these patients. We recommend moderating activity to tolerable levels that do not worsen symptoms, keeping the patient’s heart rate under 110 BPM. Furthermore, patients need to identify the activity level beyond which their symptoms worsen, and then aim to stay below that level of activity. Stretching and low-level resistance exercises are preferred over aerobic exercises. -
Low Dose Naltrexone (LDN): 1-4.5 mg/day
LDN has been demonstrated to have anti-inflammatory, analgesic, and neuromodulating properties. Begin with 1 mg/day and increase to 4.5 mg/day, as required. May take 2 to 3 months to see full effect. -
Resveratrol 400-500 mg/day
This plant phytochemical (flavonoid) has remarkable biological properties and activates autophagy. A bio-enhanced formulation containing trans-resveratrol from Japanese Knotweed Root appears to have improved bioavailability. Quercetin acts synergistically and increases the bioavailability of resveratrol. Pterostilbene is another plant flavonoid similar to resveratrol, but with greater absorption and cellular uptake. A “high quality” combination supplement with resveratrol, quercetin, and pterostilbene is ideal. Resveratrol in a dose of 500 mg twice daily is suggested for acutely symptomatic patients. In recovered patients and those on preventative/maintenance therapy, a daily dose of 400-500 mg should suffice. The safety of these phytochemicals has not been determined in pregnancy and they should therefore be avoided. Due to the possible drug interaction between quercetin and ivermectin these drugs should not be taken simultaneously (i.e., should be staggered morning and night). For more detailed information see ‘An Approach to the Management of Post-Vaccine Syndrome‘. -
Melatonin: 2–6 mg slow release/extended release prior to bedtime
Melatonin has anti-inflammatory and antioxidant properties and is a powerful regulator of mitochondrial function. The dose should be started at 750 mcg (μg) to 1 mg at night and increased as tolerated. Patients who are slow metabolizers may have very unpleasant and vivid dreams with higher doses. -
Aspirin: 81 mg/day
-
Probiotics/prebiotics
Patients with post-vaccine syndrome classically have severe dysbiosis with loss of Bifidobacterium. A no-sugar-added, Greek yogurt with both pre- and probiotics is recommended. Suggested probiotics include Megasporebiotic (Microbiome labs), TrueBifidoPro (US Enzymes) and yourgutplus+. Depending on the brand, some pro/prebiotic products can be very high in sugar, which promotes inflammation, so read labels carefully. -
Spermidine: 1000-2000 mg (wheat germ extract)/daily
Spermidine is a naturally occurring polyamine that, like resveratrol, has anti-inflammatory and antioxidant properties. It preserves mitochondrial function and has been shown to reduce cardiovascular disease, and all-cause mortality, prolong lifespan and promote autophagy. Wheatgerm, mushrooms, grapefruit, apples, and mango are high natural sources of spermidine. Wheatgerm supplements contain high amounts of spermidine with good bioavailability. For more detailed information and important contraindications see ‘An Approach to the Management of Post-Vaccine Syndrome‘. -
Sunlight and Photobiomodulation (PBM)
PBM is also referred to as low-level light therapy, red light therapy, and near-infrared light therapy. Of all the wavelengths of sunlight, near-infrared radiation (NIR-A) has the deepest penetration into tissues. NIR-A in the range of 1000 to 1500 nm is optimal for heating tissues. For more detailed information see ‘An Approach to the Management of Post-Vaccine Syndrome‘.
Adjunctive/Second-Line Therapies
(Listed in order of importance.)
-
Methylene Blue:
Methylene blue (MB) has a number of biological properties that may be potentially beneficial in vaccine-injured patients. MB induces mitophagy (mitochondrial autophagy) and has anti-inflammatory, antioxidant, neuroprotective, and antiviral properties. MB and photobiomodulation (PBM) have similar beneficial effects on mitochondrial function, oxidative damage, and inflammation, and the two treatments are often combined.Low-dose MB is a therapeutic option in patients with brain fog and other neurological symptoms. Patients or their healthcare providers need to purchase high-quality methylene blue powder and formulate an orally administered 1% solution (10 mg MB in 1 ml of water). To achieve this, mix 1 gram of methylene blue powder with 100 ml of water.
Use a dropper bottle to administer — 1 drop of 1% solution is approximately 0.5 mg of methylene blue).
Dosing of LDMB:
- Start with 5 mg (.5 ml or 10 drops) twice daily for the first week.
- Then gradually increase the dosage every 2-3 days (guided by symptoms – i.e., improvement in fatigue and/or cognitive improvement) until you reach a maximum of 30 mg (3 ml) per day.
- Take the 7th day off every week to allow the body to “reset”.
The optimal dose is highly individualized and each patient needs to find the right dose for them.
LDMB will cause your urine to be blue or blue-green, and may stain teeth. Some patients may experience a Herx reaction. A Herx reaction may cause fatigue, nausea, headache, or muscle pain. If you experience a Herx reaction, stop the protocol for 48 hours and then resume again slowly.
DO NOT take MB if you are pregnant or breastfeeding.
-
Nigella Sativa: 200-500 mg encapsulated oil twice daily
For more detailed information and important contraindications see ‘An Approach to the Management of Post-Vaccine Syndrome‘. -
Vitamin C: 1000 mg orally three to four times a day
Vitamin C has important anti-inflammatory, antioxidant, and immune-enhancing properties, including increased synthesis of type I interferons. Avoid in patients with a history of kidney stones. Oral Vitamin C helps promote growth of protective bacterial populations in the microbiome. -
Vitamin D and Vitamin K2: A dose of 4000–5000 units/day of Vitamin D, together with Vitamin K2 100 mcg/day is a reasonable starting dose.
The dose of Vitamin D should be adjusted according to the baseline Vitamin D level. -
Fluvoxamine: 50 mg twice daily
Start on a low dose of 12.5 mg/day and increase slowly as tolerated. NOTE: Some individuals who are prescribed fluvoxamine experience acute anxiety, which needs to be carefully monitored for and treated by the prescribing clinician to prevent rare escalation to suicidal or violent behavior. -
Magnesium: A starting dose of 100 to 200 mg daily is suggested, increasing as tolerated up to 300 mg to 400 mg daily.
There are at least 11 different types of magnesium that can be taken in supplement form with varying bioavailability. Generally, organic salts of Mg have a higher solubility than inorganic salts and have greater bioavailability. See ‘An Approach to the Management of Post-Vaccine Syndrome‘ for further information and important dosing precautions. -
Omega-3 Fatty Acids: We suggest a combination of EPA/DHA with an initial dose of 1 g/day (combined EPA and DHA) and increasing up to 4 g/day (of the active omega-3 fatty acids).
-
Non-Invasive Brain Stimulation (NIBS):
NIBS using transcranial direct current stimulation or transcranial magnetic stimulation has been demonstrated to improve cognitive function in patients with long COVID as well as other neurological diseases. NIBS is painless, extremely safe, and easy to administer. It is a recognized therapy offered by many Physical Medicine and Rehabilitation Centers. Patients may also purchase an FDA-approved device for home use. -
N-acetyl cysteine (NAC): 600-1500 mg/day
NAC, the precursor of reduced glutathione, penetrates cells where it is deacetylated to yield L-cysteine, thereby promoting GSH synthesis. Oral administration of NAC likely plays an adjuvant role in the treatment of the vaccine injured. Oral Glutathione is poorly absorbed and is therefore not recommended. A combination supplement that contains acetyl glutathione, NAC and Vitamin C may enhance the bioavailability of glutathione. -
Cardio Miracle™ and L-arginine/L-citrulline supplements
Cardio Miracle is a supplement with over 50 ingredients formulated to increase nitric oxide (NO) production. The supplement contains L-arginine, L-citrulline, Beetroot (high in dietary nitrates), L-Ornithine, CoQ10, as well as a blend of fruit and vegetable phytonutrients. -
Sildenafil with or without L-arginine-L-Citrulline: doses titrated up from 25 to 100 mg 2-3 times daily with L-arginine/L-citrulline powder twice daily
May be helpful for brain fog as well as microvascular disease with clotting and poor perfusion. It is noteworthy that curcumin, resveratrol, EGGG, and valproic acid all potentiate phosphodiesterase 5 (PDE5) inhibitors. -
Intravenous Vitamin C: 25 g weekly, together with oral Vitamin C 1000 mg (1 gram) 2–3 times per day.
High-dose IV vitamin C is “caustic” to the veins and should be given slowly over 2–4 hours. Furthermore, to assess patient tolerability the initial dose should be between 7.5–15 g. Total daily doses of 8–12 g have been well-tolerated, however chronic high doses have been associated with the development of kidney stones, so the duration of therapy should be limited. Wean IV Vitamin C as tolerated. -
Hydroxychloroquine (HCQ): 200 mg twice daily for 1-2 weeks, then reduce as tolerated to 200 mg/day
HCQ is a potent immunomodulating agent and is considered the drug of choice for systemic lupus erythematosus (SLE), where it has been demonstrated to reduce mortality. Thus, in patients with positive autoantibodies or where autoimmunity is suspected to be a prominent underlying mechanism, HCQ should be considered earlier. Note: HCQ will limit the effectiveness of intermittent fasting. -
Low Dose Corticosteroid: 10–15 mg/day prednisone for 3 weeks. Taper to 10 mg/day and then 5 mg/day, as tolerated.
-
Mitochondrial Energy Optimizer with pyrroloquinoline quinone (e.g., Life Extension Energy Optimizer or ATP 360®).
-
Behavioral Modification, Relaxation Therapy, Mindfulness Therapy, and Psychological Support
May help improve patients’ overall well-being and mental health. Suicide is a real problem in vaccine-injured patients. Support groups and consultation with mental health professionals are important. Tai Chi, a health-promoting form of traditional Chinese martial art, has been shown to be beneficial for preventing and treating diseases including long COVID. Yoga has immunomodulating properties that may be beneficial in vaccine-injured patients.
Third Line Therapies
-
Hyperbaric Oxygen Therapy (HBOT):
HBOT has potent anti-inflammatory properties, decreasing pro-inflammatory cytokines while increasing IL-10. Furthermore, HBOT polarizes macrophages toward the M2 phenotype and improves mitochondrial function. Surprisingly, it is the increased pressure, rather than the increase in the concentration of dissolved oxygen, that appears to mediate these effects. Please refer to ‘An Approach to the Management of Post-Vaccine Syndrome‘ for treatment information, references, and other important details. -
Low Magnitude Mechanical Stimulation (LMMS or Whole-Body Vibration).
Low-magnitude (0.3-0.4G), high-frequency (32-40 Hz) mechanical stimulation has been demonstrated to increase bone density as well as indices of general well-being in patients with a variety of medical disorders. This therapy is offered by Physical Medicine and Rehabilitation Centers, or a device may be purchased for home use (https://www.juvent.com/health) similarly with noninvasive brain stimulation (NIBS).
-
Patients with Elevated Homocysteine Levels:
Such patients may benefit from treatment with 800 ug of 5-methyl tetrahydrofolate (5-MTHF), the most biologically active form of folic acid. Supplementation with folic acid alone will paradoxically increase homocysteine levels, particularly in patients with MTHFR polymorphism. In addition, B complex vitamins containing B2 (riboflavin) and Vitamin B6, magnesium, and Vitamin D should be added.
-
Other Potential Treatments
(Limited data/Require further evaluation; see ‘An Approach to the Management of Post-Vaccine Syndrome‘ for more information)
- Plasmapheresis
- Valproic acid; Depakote, 250 mg 2-3 times daily
- Induced hyperthermia and Cold Hydrotherapy
- Pentoxifylline (PTX); PTX ER, 400 mg three times daily
- Maraviroc; 300 mg orally twice daily
- Sulforaphane (broccoli sprout powder); 500 mcg–1g twice daily
- Dandelion (Taraxacum officinale); 4-10 g three times daily (20-30 mg/ml in hot water)
- VEDICINALS® 9
- C60 or C60 fullerenes
- Intravenous immunoglobulin (IVIG) treatment
- Immunosuppressive therapies
Table 1. How to calculate ivermectin dose
| How much do I weigh? | What dose does the protocol say? | ||||
|---|---|---|---|---|---|
| In pounds | In kilograms | 0.2 mg/kg: | 0.3 mg/kg: | 0.4 mg/kg: | 0.6 mg/kg: |
| 70-90 | 32-41 | 6-8 mg | 10-12 mg | 13-16 mg | 19-25 mg |
| 91-110 | 41-50 | 8-10 mg | 12-15 mg | 17-20 mg | 25-30 mg |
| 111-130 | 50-59 | 10-12 mg | 15-18 mg | 20-24 mg | 30-35 mg |
| 131-150 | 60-68 | 12-14 mg | 18-20 mg | 24-27 mg | 36-41 mg |
| 151-170 | 69-77 | 14-15 mg | 21-23 mg | 27-31 mg | 41-46 mg |
| 171-190 | 78-86 | 16-17 mg | 23-26 mg | 31-35 mg | 47-52 mg |
| 191-210 | 87-95 | 17-19 mg | 26-29 mg | 35-38 mg | 52-57 mg |
| 211-230 | 96-105 | 19-21 mg | 29-31 mg | 38-42 mg | 58-63 mg |
| 231-250 | 105-114 | 21-23 mg | 32-34 mg | 42-45 mg | 63-68 mg |
| 251-270 | 114-123 | 23-25 mg | 34-37 mg | 46-49 mg | 68-74 mg |
| 271-290 | 123-132 | 25-26 mg | 37-40 mg | 49-53 mg | 74-79 mg |
| 291-310 | 132-141 | 26-28 mg | 40-42 mg | 53-56 mg | 79-85 mg |
This protocol is solely for educational purposes regarding potentially beneficial therapies for COVID-19. Never disregard professional medical advice because of something you have read on our website and releases. This protocol is not intended to be a substitute for professional medical advice, diagnosis, or treatment with regard to any patient. Treatment for an individual patient should rely on the judgement of a physician or other qualified health provider. Always seek their advice with any questions you may have regarding your health or medical condition. Please note our full disclaimer at: www.flccc.net/disclaimer
___
https://covid19criticalcare.com/treatment-protocols/i-recover/