
ARPA-H, a branch of the IC within NIH
I really did not begin to understand the Washington DC/Bethesda- based National Institutes of Health (NIH) healthcare bureaucracy until my research laboratory was recruited and relocated from the University of California, Davis to the University of Maryland, Baltimore School of Medicine in 1997. Before then, I had a vague notion that the NIH intramural (Bethesda/Rockville- based research campus) and extramural (mostly Rockville administrative campus) infrastructure was a sort of research paradise, where all the really important government funded biomedical research work was done. For the lucky few who were good enough, the elite of the elite, they were able to work unencumbered by the daily grind of the endless begging-for-dollars grant and contract writing (and associated funding politics) which has come to dominate the lives of most academic biomedical researchers.
After Jill and I relocated the lab to Baltimore’s inner harbor, I realized that the U MD, Baltimore campus had become sort of a satellite to the Bethesda NIH complex, and I started being asked to make presentations and participate in “study sections” – one step along the “peer review” process of selecting which research gets funding and which will wither on the vine. The process of how that sausage making machine actually works is another story, but suffice to say that it is nothing like what people are lead to believe. “Peer review” is largely a sham, and what and who actually gets funded is pretty much completely at the whim of the top bureaucrats that run the place (Dr. Fauci is just one example)- who are both untouchable and unaccountable. Absent a major moral transgression scandal, they literally cannot be fired by the executive branch (which is supposed to provide oversight), and their internal government customer is essentially Congress. Which gives rise to the strategy of rigorously tracking and reporting NIH institute funding allocation by state and congressional district.
Here’s how this works. Congress allocates money to the NIH, which then gets divided into the intramural activities (internal government researchers) and extramural activities (the money that goes back to congressional districts in the form of grants and contracts). Over time, this has lead to a “you scratch my back, I’ll scratch yours” feedback loop of taxpayer-funded (or borrowed) money. Not at all what the administrative and technical genius Vannevar Bush had envisioned when he lead the creation of the Office of Scientific Research and Development (OSRD) in 1941. OSRD, born of the war effort, essentially became the granddaddy of the entire federal scientific research enterprise- including NIH, and neither congress nor the executive branch have ever looked back to assess if the American people are getting good value.
The objectivity of the sycophant journalists and corporate press (the Washington Post and New York Times provide notable examples) that should be examining and exposing this circle jerk is compromised by the same problem that lead to their not reporting on the mortgage loan malfeasance that resulted in the financial meltdown of the “Great Recession” of 2007-2009. The conflict of interest which drives the curious myopia of the fourth estate in such matters has been elegantly described in the blockbuster movie “The Big Short”. Here’s how that one works. If you are a journalist covering the healthcare beat, and wish to have access to the inside “scoops” concerning what is going on or coming up within the US Government “health” bureaucracy, you need to have insider access. You want to be on the list of people that are contacted concerning an upcoming press release or emerging issue. But the quid pro quo is that you have to play nice with the big boys, and not be too critical (see “controlled opposition” or “Hegelian dialectic”) or you will lose access to the centers of power and associated information stream. For an excellent example illustrating how Drs. Fauci, Collins and peers have learned to manipulate this reciprocal relationship with the press to advance their own power and political agendas, see their emailsconcerning the authors of the Great Barrington Declaration.
Over the ensuing 80 years, the whole thing has become a self-perpetuating and ever expanding bureaucratic monster which is so deeply woven into the fabric of government that it may never be possible to re-imagine or reform the beast. After all, who does not support better health care? Who knows better than the “experts” who lead the bureaucracy? Any congressperson or executive branch political appointee (or heretic physician/scientist) who dares to question is attacked, gaslighted, and vilified by both the bureaucrats themselves and the corporate-controlled press. This bureaucratic “healthcare” enterprise has become untouchable, and has been further entrenched by building “public-private partnerships” (essentially corporatism by another name) with the medical-industrial complex. Never mind the fact that this feedback loop of self interest has spawned one of the most expensive health care systems in the world, and that the overall health and longevity of the American taxpayers who fund it continues to slip, year by year, down the ladder of world health outcome ranking.
I am searching my brain for the right metaphor to express the reality of the NIH that I actually encountered in moving from the academic epicenter of California agriculture to the belly of the medical-industrial complex beast – an astronomic Black Hole comes closest. Like the effects of a Black Hole on spacetime, the massive amount of money allocated to the NIH bureaucracy by the US Federal Government (year, after year, after year) distorts every aspect of modern medical research, across the United States medical research enterprise and beyond throughout the world.
So with that prelude and context, enter the new NIH program called ARPA-H (Advanced Research Projects Agency for Health). The 6.5 billion dollar (initial budget) program was created by Dr. Francis Collins and White House Office of Science and Technology Policy Director Eric S. Lander during the current Biden administration, ARPA-H is so new that it has yet to be assigned to one of the 27 NIH institutes and centers, and in the interim during this formation phase resides within the Office of the Director of NIH (Director, Dr. Elias A. Zerhouni). A cool Billion for 2022 has already been transferred into the program, even though it is not really operating yet. As they say in DC, a Billion here, a Billion there, and pretty soon it adds up to real money ($45 billion this year for NIH, give or take, according to the accounting summarized here). Of course, that does not include the monies for related organizations like the Biomedical Advanced Research and Development Authority (BARDA) (a mere $1.6 Billion) or the entire FY2022 budget of the office of the Assistant Secretary for Preparedness and Response (ASPR- $3.3 Billion including BARDA).
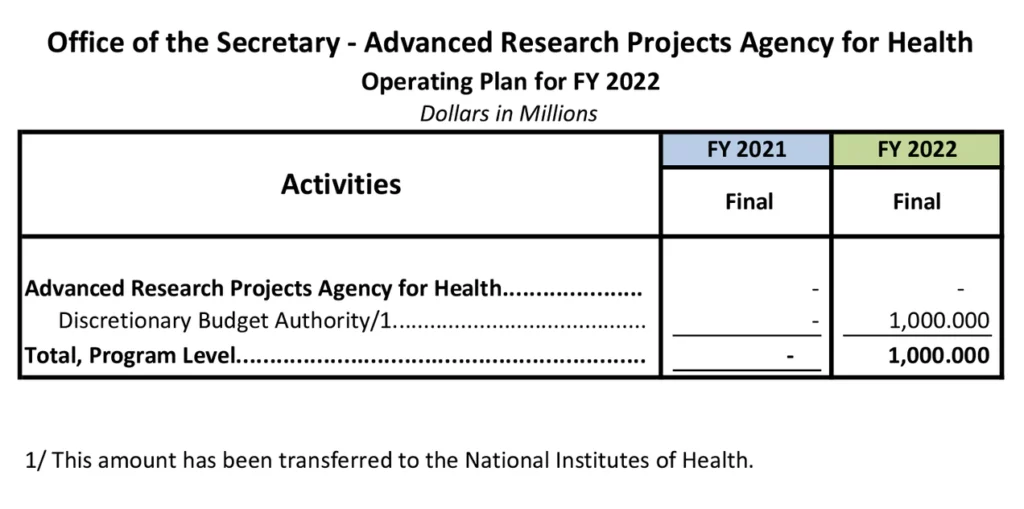
(Nice detail on that budget breakdown, by the way!)
Now, just to provide context, ASPR has operational responsibilities for the advanced research, development and stockpiling of medical countermeasures as well as the coordination of the Federal public health and medical response to emergencies and disasters. ASPR/BARDA funds development and purchase/stockpile all of the vaccines, drugs, respirators etc. to meet the nations biodefense needs, for a cost of $3 Billion plus change. So, what is the mission which ARPA-H is going to fulfill for a bit less than 1/3 of that budget? According to it’s own website:
“The proposed mission of ARPA-H could be to make pivotal investments in break-through technologies and broadly applicable platforms, capabilities, resources, and solutions that have the potential to transform important areas of medicine and health for the benefit of all patients and that cannot readily be accomplished through traditional research or commercial activity.
ARPA-H will:
Speed application and implementation of health breakthroughs to serve all patients
Foster breakthroughs across various levels — from the molecular to the societal
Build capabilities and platforms to revolutionize prevention, treatment, and cures in a range of diseases
Support “use-driven” ideas focused on solving practical problems that advance equity and rapidly transform breakthroughs into tangible solutions for all patients.
Focus on multiple time-limited projects with different approaches to achieve a quantifiable goal.
Use a stage-gate process, with defined metrics, and inject accountability through meeting these metrics.
Overcome market failures through critical solutions or incentives
Use the Defense Advanced Research Projects Agency (DARPA) as a model to establish a culture of championing innovative ideas in health and medicine.”
Could be. In the investment community, that would be called a “non-binding forward looking statement”. As I read it, the mission of ARPA-H is (maybe? could be?) to do what NIH, with its’ $45 billion per year in funding, is failing to accomplish. How, you ask? Apparently by mimicking the way that the infamous Defense Advanced Research Projects Agency (DARPA) is run, and trying to transplant a bit of entrepreneurial spirit into NIH. And to be able to employ alternative contracting mechanisms to engage with the Medical-Industrial complex such as the “Other Transactional Authority” (OTA) mechanism used to bypass the Federal Acquisition Regulations. By the way, Pfizer has nicely exploited the OTA to build yet another way to shield themselves from any liability incurred with their COVID mRNA vaccine program. Sounds great – what could possibly go wrong <sarcasm>?
This Bloomberg interview of Francis Collins may be among the most helpful in trying to figure out what is really being planned for the initial $6.5B ask. Although when I called in to the Office of the Director of NIH to try to get clarity on which part of the bureaucracy was going to get dominion over the budget I was told that the decision had not yet been made, but in this interview Francis Collins seems pretty sure he knows the answer-
“What kind of person are you looking for to lead ARPA-H?
A very entrepreneurial person who has experience in moving forward projects that are high risk, but high reward, and quickly. Maybe somebody who also is experienced with failure, because we want to be sure we know how to see that when it’s coming and make decisions quickly. Most likely, this will be somebody from the private sector, or at least somebody who’s had significant private sector experience.
The ARPA-H head would have a reporting line to the NIH director, who would need to be pretty hands off as far as interfering with the decision process and what projects to pursue, but very hands on in terms of providing the kind of administrative support that’s going to be necessary to get this agency started as quickly as possible.
There is a debate going on about whether this should be a presidential appointment. The weight of evidence would say no because then it starts to seem political. And there might be risks involved there, so they will probably be appointed by the health and human services secretary.”
Cutting through the chaff here, what I read is basically that 1) NIH is way too slow and kludgy (it often takes five years from initial scientific funding concept to getting money out the door). 2) DoD/DARPA, which Fauci and others have criticized as not getting the biodefense job done (but remember that DARPA would not fund the EcoHealth Alliance coronavirus gain of function research at the Wuhan Virology lab which Fauci funded!), is running circles around NIH. 3) BARDA is not able to get the job done either (there is a big overlap between ARPA-H and the BARDA mission.) 4) Collins wants this money to come to the Office of the Director, NIH. 5) Collins does not want the director of ARPA-H to be accountable to the President/Executive Branch. 6) Collins wants the NIH to be more able to compete with private sector efforts (“this will be somebody from the private sector”).
Furthermore, based on the ARPA-H website, it looks to me like biometric identification is going to be a big focus here, and it is a reasonable possibility that this will be the center that will have ownership of driving forward various aspects of the Transhumanism agenda for the civilian sector, potentially to include DNA-based identification technologies.
This basically overlaps with the same mission and logic used to justify the NIAID Vaccine Research Center (VRC), which is the group that partnered with Moderna to create that mRNA COVID vaccine (resulting in a nice patent royalty stream from the federal investment for all concerned). The general wisdom applies yet again. When the current funding and bureaucracy is not getting the job done, add more money and bureaucracy. How is ARPA-H different?
To get a peek under the bureaucratic skirts so that we can better understand what is really going on here (“you will know them by their actions, not by their words”), it could be useful to examine who is the brilliant entrepreneurial spirit who has been grabbed out of a leading biomedical innovator corporation to inject a bit of chutzpa into the ossified NIH bureaucracy. Well, thanks to a HHS press release, the mystery has been resolved:
“Health and Human Services Secretary Xavier Becerra today announced the formal establishment of the Advanced Research Project Agency for Health (ARPA-H) as an independent entity within the National Institutes of Health and the appointment of Adam H. Russell, D.Phil., as acting deputy director. Currently, Dr. Russell is the Chief Scientist at University of Maryland’s Applied Research Laboratory for Intelligence and Security (ARLIS). He spent more than a decade as a Program Manager, first at the Intelligence Advanced Research Projects Activity (IARPA) and then at the Defense Advanced Research Projects Agency (DARPA). Dr. Russell will begin his new role in June.
With broad technical and management experience across several disciplines, ranging from cognitive neuroscience and physiology to cultural psychology and social anthropology, Dr. Russell will guide the early stages of building the administrative structure of the agency and oversee the hiring of initial operational staff to ensure the agency is stood up as effectively and efficiently as possible. President Biden will appoint an ARPA-H Director who will be responsible for administration and operation of ARPA-H and will report to the HHS Secretary.
“We are ecstatic that Dr. Adam Russell has accepted the challenge to help launch ARPA-H, President Biden’s bold, new endeavor to support ambitious and potentially transformational health research in this country,” said Secretary Becerra. “ARPA-H will have a singular purpose: to drive breakthroughs in health, including the prevention, detection and treatment of diseases such as cancer, Alzheimer’s and diabetes.”
Dr. Russell joined DARPA as a Program Manager in July 2015. His work there focused on new experimental platforms and tools to facilitate discovery, quantification and “big validation” of fundamental measures in social science, behavioral science and human performance.
Before joining DARPA, he was a Program Manager at IARPA, where he developed and managed a number of high-risk, high-payoff research projects for the Office of the Director of National Intelligence. Prior to IARPA, Dr. Russell was in industry, where he was a senior scientist and principal investigator on a wide range of human performance and social science research projects and provided strategic assessments for a number of different government organizations.
Dr. Russell holds a Bachelor of Arts in Cultural Anthropology from Duke University, and an M.Phil. and a D.Phil. in Social Anthropology from Oxford University, where he was a Rhodes Scholar.”
Here is Dr. Russell’s U Maryland bio, which is even more revealing.
“Dr. Adam Russell is a research scientist at UMD’s Applied Research Laboratory for Intelligence and Security (ARLIS), with an adjunct faculty position in UMD’s Department of Psychology. Adam began his career in national security working on human performance and strategic competitions for various government organizations. After joining the government in 2009, he spent the next decade as a Program Manager at the Intelligence Advanced Research Projects Activity (IARPA) and then the Defense Advanced Research Projects Agency (DARPA) – where he was known as the “DARPAnthropologist.” At IARPA and DARPA, Adam managed a large portfolio of high-risk, high-impact R&D programs focused on enhancing the USG’s Human Domain capabilities to better understand, anticipate, and leverage human social behavior and variability through improving scientific discovery, innovation, and reproducibility, especially in the social and behavioral sciences (e.g., Next Generation Social Science (NGS2), Collective Allostatic Load, Systematizing Confidence in Open Research and Evidence (SCORE), Ground Truth, How the Social Becomes the Biological, Strengthening Human Adaptive Reasoning and Problem-solving (SHARP), Tools for Recognizing Useful Signals of Trustworthiness(TRUST), and ODNI and IARPA’s first public data analysis incentive “Challenge” competition, INSTINCT). “
A PhD anthropologist with industrial experience in “human performance and social science research projects” who has spent years as a bureaucrat-administrator at IARPA and then DARPA, and whose most recent appointment was at the University of Maryland Applied Research Laboratory for Intelligence and Security . I certainly do not see someone selected to “revolutionize how to prevent, treat, and even cure a range of diseases including cancer, infectious diseases, Alzheimer’s disease, and many others that together affect a significant number of Americans.”
Frankly, what I see is yet another spook being strategically placed into the federal side of the “public-private partnership” which exists between the global medical-industrial complex and the US federal government, and given a nice juicy $6.5B birthday gift with no strings attached and no ability of the executive branch to provide oversight. ARPA-H appears to me to be an intelligence community operational research arm that has been embedded into the Office of the Director of NIH. What could possibly go wrong?
When will they ever learn.
(PS: Anyone know if Dr. Adam Russell is related to Major General Dr. Philip Russell?)
___
https://rwmalonemd.substack.com/p/arpa-h-a-branch-of-the-ic-within