
When a Vaccine Kills More than it Cures
Submitted by TP
- COVID-19 virus has not been isolated or purified
- Named variants such as Delta are waves of outbreaks, not subtypes of the virus
- PCR tests do not indicate a person is infected with active virus
- PCR cases are not cases of active infection
- PCR tests have a high false positive rate that varies with the lab-cycle rate, over 24 is useless
- PCR lab-cycle rates of 35+ cycles have 97% false positive rates
- Cycle rates for PCR tests in laboratories can be increase to manufacture outbreaks
- PCR test kits were ordered by governments from 2017
- Mild to moderate cases are best treated with Ivermectin
- Primary prevention programmes could use Ivermectin instead of vaccines
- Real vaccines contain live attenuated virus
- Real vaccines undergo extensive clinical trials before release
- mRNA experimental medications are not Vaccines
- Natural immunity lasts longer and is more effective than vaccine immunity
- Natural immunity produces antibodies
- Antibodies can be found in the blood
- Blood screening would identify those that are naturally immune
- Naturally immune persons do not require vaccination
- Natural immunity is being ignored
- Asymptomatic PCR positive cases are not infective
- Masks don’t work
- Social isolation prevents natural immunity
- Vaccination side effects are grossly underreported
- Vaccination deaths are suppressed
- Postmortems on vaccine related deaths are non-existent
- Consents are supposed to be fully informed
- Fully informed, requires completed clinical trials
- Menstrual irregularities reflect disordered ovulation
- Sperm may be affected as well
- Overall fecundity will be reduced restricting population regeneration
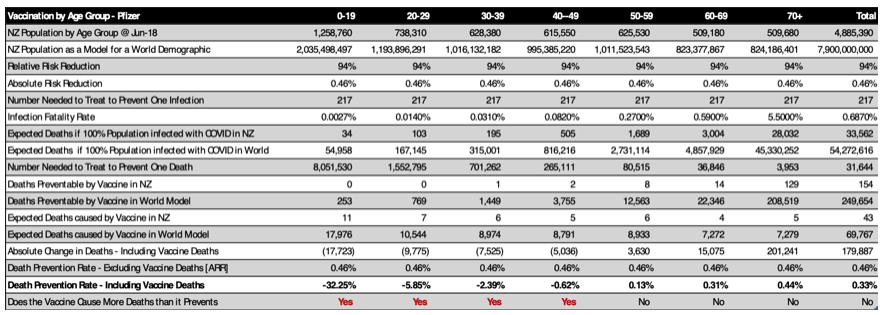
So, let’s check the figures to see if the vaccines do more harm than good. A randomized controlled clinical trial1 has provided the following relative risk reduction rates [RRR] and absolute risk reduction rates [ARR]. An observational study out of Israel2 has comparable [RRR] real life results for Pfizer-BioNTech. The ARR varies from 0.46% (Pfizer) to 1.3% AstraZeneca. The number needed to treat to prevent one infection [NNT = 1/ARR] varies from 77 to 217 persons. Once we know the NNT to prevent one infection we can calculate the NNT to prevent one death [mNNT] from the infection fatality rate [IFR]. This is available from a study3 in pre-print on medRxiv:

Using the New Zealand population as a demographic and expanding the results to a World model, whilst using the ARR above, yields the following expected outcomes for the Pfizer vaccination programme in New Zealand:
- The infection fatality rate increases with age and is highest in the over 70 age group.
- Gene therapy does not discriminate by age and affects all ages, especially the large population of the under 20 age group.
- Reports are emerging in New Zealand of a greater than expected number of deaths from the Pfizer vaccination programme.
- There are community gathered database reports of 100+ vaccine related deaths, with only one death reported publicly by the government.
- The vaccine appears to be of little benefit with an overall death prevention rate of 0.33 of one percent.
- There appears to be no benefit below the age of 50 and minimal benefit beyond.
- Those under 50 and especially the those under 20 years of age should avoid the vaccine due to increased mortality.
- Deaths prevented by the vaccine do not exceed deaths caused by the vaccine until over 50 years of age.
- The only group where there is an acceptable risk to reward ratio is the 70+ age group.
- Those vaccinated in the 70+ age group still have a risk of death comparable to the non-vaccinated.
- Hospitalisation rates should be similar for the vaccinated and unvaccinated.
- Unless, the reported vaccine death cases are grossly under reported, then the vaccine related hospitalisations and deaths would be higher.
- Delta outbreak post vaccination hospitalisations and deaths are much higher, so underreporting of vaccine deaths is highly likely.
- The ‘Death Prevention Rate – Including Vaccine Deaths’ is sensitive to (rises with) the reported number of vaccine deaths.
If the reported number of vaccine deaths increase 100-fold, as suggested by the New Zealand citizens database:
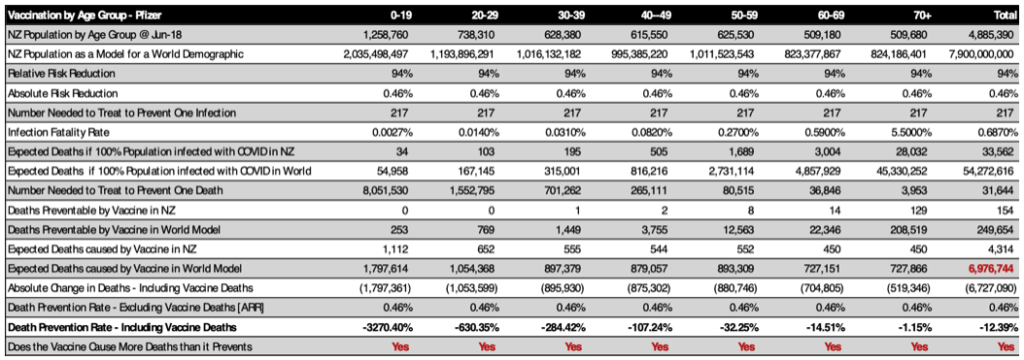
- The expected deaths caused by the vaccine now far exceed the virus infection fatality rate in the unvaccinated; they ARE manufactured pandemic deaths.
- Now there is no age group in which the vaccine has a positive effect on death prevention.
- There is now a distinct increase in vaccine related deaths in the fertile age female population, as opposed to just the under 20 age group.
There are many reports of menstrual irregularities post vaccination:
- Menstrual irregularities are a clinical sign of disordered or absent ovulation.
- A study on pregnancy related effects of the vaccine cleverly mixed late pregnancy results [mainly unaffected] with early (first trimester) results [mostly affected]4.
- The concealed spontaneous miscarriage rates in the first trimester [37-44/81 T1 vaccine cases5] are between 46-54% post vaccination [normal 10%].
- Male fertility may also be reduced by the vaccine affecting healthy sperm production.
- The overall affect would be to reduce the ability of the population to reproduce and recover the population.
If 100% vaccination rates are achieved there will be no comparison group left and all deaths can then be blamed on the Virus with no way of proving otherwise.
Given the vast number of Ivermectin RCTs with positive results for primary prevention, why would we continue with this vaccination programme:

*References in Links
References:
- Olliaro P, Torreele E, Vaillant M: COVID-19 vaccine efficacy and effectiveness—the elephant (not) in the room, Lancet Microbe. 2021; published online April 20, https://doi.org/10.1016/S2666-5247(21)00069-0.
- Dagan N, Barda N, Kepten E, et al. BNT162b2 mRNA COVID-19 vaccine in a nationwide mass vaccination setting. N Engl J Med 2021; published online Feb 24, DOI: 10.1056/NEJMoa2101765.
- Axfors C, Ioannidis J: Infection fatality rate of COVID-19 in community-dwelling populations with emphasis on the elderly: An overview, Meta-Research Innovation Center at Stanford (METRICS), Stanford University, Stanford, California, USA, Departments of Medicine, of Epidemiology and Population Health, of Biomedical Data Science, and of Statistics, Stanford University, Stanford, California, USA; medRxiv. 2021; published online July 13 at, https://doi.org/10.1101/2021.07.08.21260210.
- Shimabukuro T, et al: Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. N Engl J Med 2021; published online April 21, 384:2273-2282
DOI: 10.1056/NEJMoa2104983. - Shimabukuro T, et al: Supplementary Appendix to Ref 4.